A quick overview of a few crucial research conclusions to keep in mind for allergic children.
By: MRS Allergy Medical Director Dean C. Mitchell, MD, Board Certified Immunologist and author of Allergy & Asthma Solution
Every pediatric practice sees its share of allergic children every day. Common conditions range from food allergies to eczema, rhinitis and asthma. It’s not easy to keep up with the latest findings in every area of pediatrics, so I feel compelled to share with our MRS pediatric practices the key studies that ought to be familiar to all pediatricians.
Peanut Allergy Prevention: The LEAP Study
In 2015, a team of allergy experts reviewed the scientific literature and came forth with new recommendations for pediatricians in advising the parents of children with potential food allergies. The LEAP study, which stands for Learning Early About Peanut Allergy, turned on its head the prior common advice on trying to prevent peanut allergy. For many years, its seemed to make sense to advise parents who had other children with food allergies, especially peanut allergy, to avoid eating peanuts during pregnancy and surely to avoid feeding peanuts or peanut butter to her new child for as long as possible–hoping this avoidance would make later ingestion of peanuts a non-issue. This approach failed fairly spectacularly. The work by Gideon Lack, an allergist in Britain, showed just the opposite: introduction of peanut protein into a child’s diet as early as 4 months can significantly decrease the risk of peanut allergy.1
Practical points to implement in your practice:
- Infants 4-6 months of age who have a history of severe eczema, egg allergy or both should be blood tested (not skin tested) for peanut allergy. If they are mildly or moderately reactive but have no history of clinical, real life reactions, then slowly introduce peanut butter into their diet and monitor. If they have a strong test reaction they should not have peanut in their diet.
- Infants with mild to moderate eczema should also be blood tested for peanut reactivity, but the threshold to go ahead and give peanut butter is much lower.
- Infants without any eczema or any food allergy should have peanut introduced into the diet with other solid foods–no testing necessary.
Early Asthma Diagnosis and Early Asthma Treatment
Pediatricians are asked all the time by worried parents: does my child’s wheezing mean he or she will have asthma for life? Fernando Martinez, a professor of pulmonary medicine at Arizona University Medical Center in Tucson, set out to answer that question. He and his team identified several key factors in children who chronically wheezed before the age of seven that predict chronic asthma in later life:2
- Family history of asthma. Family history in general is predictive, but in fact, a history of maternal asthma is the best predictor of whether a a child’s wheezing will turn into chronic asthma.
- Eczema is also a key finding whether a child will develop asthma.
- Positive allergy skin tests to airborne or food allergies.
- Elevated total IgE is also an indicator.
Blocking The Allergic March and Reversing Asthma
I know that no pediatrician wants to give parents the bad news that their child, a chronic wheezer, has a higher risk for lifelong asthma. The good news is that there are things we can do to prevent that outcome. New research is clearly showing that you can prevent these high risk children from developing asthma–and you can even reverse allergic asthma! In my book, Dr. Dean Mitchell’s Allergy and Asthma Solution, I cite two key studies that show sublingual allergy immunotherapy (or allergy drops) has achieved this result.3
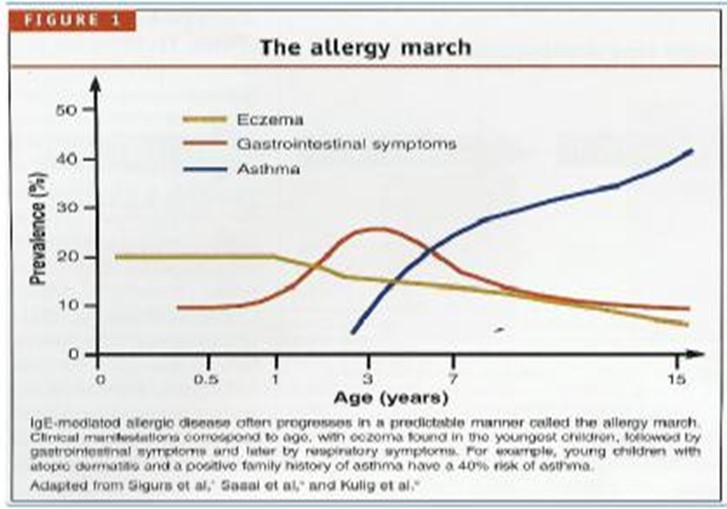
Just to review: the allergic march is the term used to refer to high risk allergic children that have food allergies and/or eczema early in life. If these conditions go goes untreated they can develop into respiratory allergies, such as asthma later in adulthood.
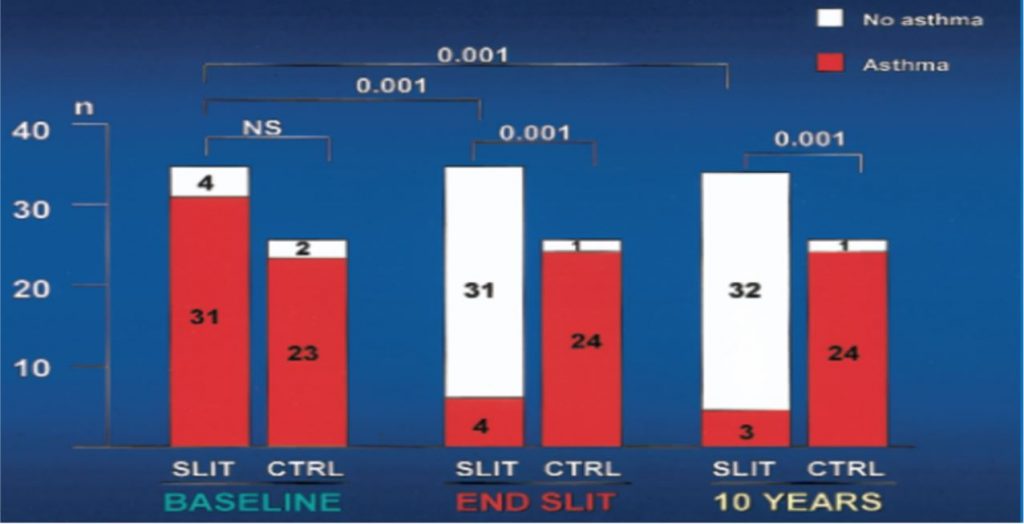
The key study I enjoy reviewing with pediatricians is by Dr. Walter Canonica, one of the world’s leading allergy researcher’s. Dr. Canonica’s study showed that young adolescents with allergic asthma could not only reverse their asthma with sublingual allergy immunotherapy and avoid the need for medications–but that it could be permanent protection!4 There is no other medical treatment that can make this claim.
The take home message is that by knowing these facts and studies you are providing your pediatric patients and their families with the latest up to date research.
MRS wants to be there to provide you with solutions for your patients.
Footnotes
1Du Toit G, et al. “Identifying infants at high risk of peanut allergy: the Learning Early About Peanut Allergy (LEAP) screening study,” J Allergy Clin Immunol 2013;131:135-43.e1
2Martinez, F. et al., “Asthma and Wheezing in the First Six Years of Life,” N Engl J Med 1995; 332:133-138. See also Morgan, W., et al, “ Outcome of Asthma and Wheezing in First 6 Years of Life,” Am J Respir Crit Care Med 2005: 172(10) 1253-1258.
3Mitchell, D, Dr. Dean Mitchell’s Allergy and Asthma Solution (Marlow & Co., 2006).
4Canonica, W.G. “Non-injection Routes of Immunotherapy.” J Allergy Clin Immunol. 2003 Mar;111(3):437-48.